The Living with HOPE Radio Show with Host Trudy Thomas will re air live NERVEmber 19th, 2015 on the Body, Mind, and Spirit Network. Due to health reasons she took leave in January and has been working toward returning.
I’ll be re-joining Trudy as co-host each Thursday at 2:30 p.m PST/5:30 p.m EST with a 30 minute guest speaker, or to review, or to discuss current affairs. The chat room will be available for your combination of listening and chatting pleasure. The call in number for the show is (929) 477-3203.
Please stay on the line to listen live or press 1 to speak to the host.
Together, we’ll bring you a diverse array of treatment options, healing essentials, technology, inspiration, activities, and living with hope.
Since 2007, Trudy’s mission has been to promote awareness for the millions of people who struggle with chronic or intractable pain. To let people know that they are not alone in their journey and that there is life after diagnosis. Trudy discusses various therapies and the emotional struggles that can arise with a chronic incurable condition such as RSD/CRPS and coming out on the other side. She strives to empower, inform and educate.
If you have a topic of interest or would like to request guest consideration and have any questions, Please, contact Trudy at: goldfield_nv@hotmail.com
With “Topic of interest” in the subject line to propose a topic. “Guest speaker” to be considered as a guest and “Question” to ask your question. Please provide your proposal or question for either. This helps filter email and requests to better serve you.
One of our original RSDS Advocates, Mary LaBree, passed away on October 15, 2015 due to complications from Reflex Sympathetic Dystrophy (RSD). Mary exemplified commitment to the RSD community for over 3 decades. As the Director of the New England RSDS Coalition since 1990, Mary sought to educate and bring awareness to the public and private sectors for the disease that was virtually unheard of back then. Originally from Leicester, Massachusetts, she was formally educated at Worcester State University in Worcester, Massachusetts.
Mary secured the JULY Proclamation for RSDS To urge all of the citizens of the Commonwealth to take cognizance of this event and participate fittingly in its observance. Given at the Executive Chamber in Boston, the twenty-fourth of June in the year two thousand and eleven, and of the Independence of the United States of America, the two hundred and thirty forth.” Massachusetts Bill # 5938
She worked both locally in Massachusetts and Nationally.
Mary formed and lead seminars, attended others, developed awareness events, distributed information and educational materials. She spoke with patients, caregivers, physicians, hospitals, insurance companies, fellow educators, universities, other peer groups, and those with an interest to learn about Reflex Sympathetic Dystrophy. She was involved with grants, research and fundraising.
When Mary LaBree began advocating for RSD in the 1980’s the term Complex Regional Pain Syndrome hadn’t been created. While other names had been used previously to describe Reflex Sympathetic Dystrophy (Syndrome) it was most often referred to as RSDS.
In 2012, she reached out to me and a friendship formed. We shared phone calls, messages and correspondence by snail mail. Mary sent me a copy of the photo of she and other’s of the original signing of her proclamation and a copy of the verbiage used to secure her proclamations. I’m privileged to know what Mary looks like. For now, I’ll not share those, nor have I ever. She shared with me 30+ years of everything. How she started, how she educated, how other RSD organizations began, her children, grandchildren, colleagues, the strength it takes to endure; not just in living with pain, but being a part of it.
If you pray, why worry… If you worry, why pray?
I had plans to meet her in person twice. The first time she had to return home early. I was supposed to meet her again toward the end of October or into mid-November. I had just spoken to her less than a week before her passing.
I was in the hospital yesterday, I had an accident with my wheelchair when I tried to back it up ( standing in front of it. ) (Stupid me )when I pushed the button to back it up.. I pushed it the wrong way..And ran over my LEDs from the ankles to the knees. I was really blessed when the ER Dr. Asked what other problems did I have, & when I explained CRPS He said oh Chronic Regional Pain Syndrome , I said yes. He treated me with kindness & care. I’m going to send him a thank you card. He was really kind. You don’t always find a kind caring Dr..pls pray for me to recover. I have a lot of CRPS work to do. I will be leaving for CA in a few weeks. Ty.M
Hi, Yes I’m looking forward to meeting you as well. I leave Oct 23 on. Friday. A lil less then 2 wks.I will call u sometime on the weekend after I arrive, hugs & lots of love.M
I’m sorry I had a mistake that I didn’t want to have a group pls forgive me, as I pressed the wrong thing, & didn’t realize it until someone told me.
The next message on Oct 12, I missed due to being away and my IM being flooded and then she was gone. I was on the road to and from the Stanford Transplant Clinic for our daughter on the 15th and in the Emergency Department on the 16th due to my cervical spine. Trying to save the puppies life all in between.
The last message was in reference to an accidental group IM.
I had been wondering if she would want to make the plans to meet at the NERVEmber, West Coast Pain Forum for Power of Pain Foundation on November 14th. All I knew for certain is she planned to be here in Northern California on the 23rd of October and would call me.
Permission granted and sent from the Power of Pain Foundation to share in Mary’s memory. Melanie McDowell Awareness and Advocacy Award Nomination 2015
I wish she would have received more nominations, but mine was the only one for her. She was most deserving.
We never know for certain where our conversations go even when we chit-chat on the phone or when we think they are in confidence. I don’t know what Mary ever spoke of me to others, but I know that she must have believed in me enough with what she did share with me to know I would keep it to me and if she didn’t know for sure when she told me she knew as time went on because I’ve never told it.
She asked me sometime in 2013 to consider being trained by her for her Coalition and new endeavors. While I was most honored, I respectfully declined as I was already committed to Power of Pain.
Our conversations also consisted of but weren’t limited to life, color, ethnicity, race, the olden days, differences, equality, change and today. She shared with me uncertainties about people, places and things, and I eased her in certain fear and prejudices. Please don’t misunderstand me, I’m not at all implying Mary was prejudice, in fact, she’s not, though conversations were simply sometimes deep. Mary listened and she learned. She watched, listened to gossip, dismissed it, listened more, read, picked it apart, put it together, and ultimately decided for herself. She wasn’t afraid to speak her mind or share a maybe, what if, what do you think or did you know.
I’m humbled to have been accepted, acknowledged, taught and even loved by her.
Mary was so proud of the New England RSDS Coalition, she was thrilled that the healthcare community was finally beginning to know what RSD (CRPS) is. She was pleased that patients had informational materials to seek out and be provided. She was happy that educational events were provided free to the public.
She told me the story behind July and why her proclamations are for the month of independence and not November. As I stated Mary began educating RSD over 30 years ago. July was chosen for freedom, freedom from pain. It wasn’t until many years later that a national color evolved, and then our month of recognition. Mary was grateful for her closest friends. I know she loved her beautiful friend, advocate and poet, Jane (Gonzales).
I prayed for her health and I prayed for her to achieve her life’s work, her mission to create awareness and educate on RSD, her purpose to continue doing so, and her hope for our future.
You did Mary! You really did! You achieved them all to the last breath.
Squirrel! But it really was. I’ve been staring out the window watching it for 30 minutes now. Running along the back fence, through the branches of the large tree that’s limbs cover the roof above my bedroom. It’s green, brown and yellow-gold leaves scattered about the ever-changing arms of fall. I gazed over as the quick little animal hurried over the Tuff Shed, back along the other side of the fence and eventually disappeared again. And then I was reminded of all the distractions.
The day before we left for the Stanford transplant center on behalf of our daughter for the second time in a month, my 6 month old puppy Independence stopped eating, drinking, became lethargic, ceased playing. No more kisses, no more loves, no greets. He’s always extremely perky, playful and active. He loves his ropes, always tugging with me, but not anymore. This was on Wednesday, the 14th that this began. We’ve already spent $2,000 saving one puppy many years ago from Parvo, nearly lost another that I was able to save by IV home care I’m not sure what’s the matter with Indie. I know, take him to the vet, but unfortunately it’s not an option. If you’ve been following any of my story relating to our daughter, no matter how much I want to and wish that I could I’m just not able.
Independence (Indie) October 6, 2015 Before he became sick.
I started force feeding him sugar-water on the 14th. Other than in the A.M. I was gone all day on the 15th and didn’t get home until nearly midnight from Palo Alto, CA. Our daughter seen her specialist and had a pre scheduled MRI immediately after. Her doctor added a brain scan as well. We drove another 20 minutes to the imaging center and learned that the scans hadn’t been authorized by the insurance. I could understand the second not being yet as it was just added, but the first hadn’t been either and had been scheduled 3 weeks prior. We signed the papers to take financial responsibility still hoping that the insurance would be approved or that we could appeal if all together denied. She has to have these scans. She was taken back and came out 15-20 minutes later in her gown into the lobby. They wouldn’t proceed without a $10,000 down payment. Oh my! Then we learned none of her Stanford appointments have been covered. Nothing we could do. She went to change and we drove back home to Sacramento.
When we got home Indie short for Independence was in the same condition as when I left. I gave him more sugar water. He wouldn’t even look at food or water. His head was droopingI rested a bit, I was exhausted, I hadn’t been feeling well, I’ve been in a flare, but my arms were hurting too much, numb, losing feeling, difficult to raise, electric shocks, my chest aching. I started researching all that I could on sick puppies. I gave him a dose of RFD Liquid Wormer for puppies and dogs and comforted him. I already had it on hand. I finally fell asleep about 4:00 a.m.
When I woke, I could barely lift my head, I couldn’t feel my arms, I could barely carry myself my back was so heavy, hate is a strong word, but I really hate the word pain, it really hurt, my collarbone area, the side of my face, my lips were having spasms and sharp spikes. All in addition to my lower back and bilateral CRPS. I was diagnosed with Fibromyalgia in 2003 also, but I know that pain enough to differentiate it from CRPS and what’s going on here. For me, Fibro feels like I’ve been run over by a truck. Really deep muscle pain. Or if I haven’t worked out in a long time, and did for a day, it’s similar to the next days muscle burn pain we get from it. My arms first started doing this a couple of years ago, lasting for over 6 months straight at one point, all day and night long in the seize and release. The only way I’ve been able to describe it is that it feels like my spinal cord stimulator is in my arms for seconds at a time. Being turned on, increasing in intensity until it reaches its peak, locks my arm up, in whatever position my arms are at the time it occurs, until the buzzing/intense tingling/shocking eases down and releases. I suppose if I didn’t have an SCS, I couldn’t describe it this way and maybe because I do I had been accidentally misleading doctors in my description. The only way to describe accurately is to truthfully describe as something feels. It’s really painful. Bringing me to tears more than a few times. I really hold back crying over my CRPS pain, I hide pain fairly well, including pain behaviors and guarding, but this has caused tear drops to rain on their own accord. Automatic. It feels like a line running through the side of my head and continuing down my neck into my arms. Worse on the right, though both are effected. And the headaches, disorientation. Phew! By the way it’s not possible for the actual stimulation from my SCS to be in my arms. Plus, back when it first occurred, I inquired to the possibility just to be sure.
Barely being able to make it down the hall because evening out my spine wasn’t an easy task, I got my coffee, and tended back to Indie. I’ve found him in the backyard twice and that scares me. I know animals often go away to pass on. He’s not an outside dog like that and because it’s not part of his normal routine it makes me uncomfortable.
I got everything ready I asked my husband to get from the store the night before. I’m bound and determined to make him better. Today is the 5th day since he’s not eaten. My husband brought back Pediatric Electrolyte, Karo Syrup, and 4 containers of chicken and rice baby food. All day long, I’m giving him a 3 ml syringe of the PediaE, 3 x each time, every hour at least. I have to pry his jaws, or attempt into the back side of his cheek between his teeth. He’s that sick. I rub the Karo on his gums to raise his blood sugar. I used a spoon to force feed him the baby food. It was messy. On the 3rd day, he finally drank water from his own bowl, but he vomited it up on my bed. Laundry! He did drink too much for not having drank in 3 days, I think. I’ve been watching for blood, there hasn’t been any that I know of. He didn’t drink any water again yesterday and he still hasn’t eaten any food and is still inactive. My 9-year-old grandson just said to me as he pet to soothe the puppy laying beside me “I miss when Indie was all hyper”.
Last evening, I added Tylenol into his daily care. I didn’t have baby Tylenol, so I put one of my Acetaminophen into a water bottle cap with a few drops of water to let dissolve. The Tylenol is a OTC 500 mg. Once liquid, I pulled approximately 150 mg of it into the syringe with the rest PediaE, shook it up, opened his mouth, and shot it down his throat and gave him 2 more 3 ml PE.
He’s so skinny.
It’s hard when you have to make choices, or rather, you don’t have any, but there are options and I’ve used my knowledge, past experiences, and the research to do as much as I can for him, as I do for the rest of my family. I hope I’m not prolonging his survival to cause him suffering but instead saving his life with all the love and compassion within me. I really don’t give up, not even on a pet.
Today I started using the syringe to get the baby food down him. Too many days have gone by. I pray I’m doing something right, he’s still hanging on.
Friday night I was diagnosed with Cervical Radiculopathy, previously diagnosed as only Paraesthesia. As long as I’m not going to drop dead of a stroke, I can figure out a way. And nope, wheels (wheelchair) are still not an option at this time. I’ve already beat being in one permanently by 10 years due to my lower extremities, not letting my upper body steal the good hard fight. Nope, not yet.
It’s taken me 2 hours to type this. A bit of a setback.
The faces and limbs in these videos are many of the people you have crossed paths with over the years. They may be your friend, colleague, or acquaintance. For other’s, you may not have realized what it is they endure. They’ve shared this part of themselves to educate and bring awareness to Reflex Sympathetic Dystrophy/Complex Regional Pain Syndrome. The faces you gaze upon seem fine, look well enough, perhaps not even a glimpse of pain, or discomfort. Such an illusion. The delusion lies less in the patient who complains than it does in the provider who doesn’t care to look beyond what initially seen. You’ll then watch the limbs of people and if you make note, you’ll find that those faces … live with more than just an ache. To see it, you have to look beyond the faces.
It’s Pain Awareness Month. Share and make aware to continue the common mission of all of us everywhere who strive to make a difference in the lives of those suffering to survive.
Uploaded on Jan 22, 2012
This is the 5th Faces of Pain video by the Power of Pain Foundation. The video contains chronic care patients who
are dealing with an autoimmune condition which attacks the nervous system, immune system, muscle, bone and
sometimes organs. For more information on the POPF or RSD please visit www.powerofpain.org. The video was
produced by Twinkle VanFleet and Kurtis VanFleet. Background Image taken by Kurtis VanFleet. This video is
property of the POPF copyright 2012. All rights reserved. The Power of Pain Foundation is a 501(C)(3) Charity.
Music
“Little Wonders” by Rob Thomas (Google Play • iTunes • AmazonMP3)
Published on Jul 12, 2012
This video goes through pictures of RSD/CRPS patients who have visual symptoms of their extremities (hands, arms,
legs and feet). RSD is a Neuro-Autoimmune condition which affects many aspects of the body. For more information
visit Power of Pain Foundation. Special thanks to Twinkle and Kurtis VanFleet, and singer Page Jackson.
Published on Aug 2, 2014
Faces of Pain Video – 6th edition for Power of Pain Foundation
Created by Twinkle VanFleet, Executive Board Member, Power of Pain Foundation
Spanish Translations by Vanessa Lara, California Representative, Power of Pain Foundation
MAKING COMPLEX REGIONAL PAIN SYNDROME SIMPLE FOR A JURY
A start-to-finish strategy for proving the chronic pain and resultant damages of CRPS
When God was testing the faith of Job, the worst punishment was physical pain…. He lost his lands and property, his family – but it was not until physical pain was inflicted that Job broke. (Job 16:6).
A case dealing with chronic pain can be difficult to prove due to the subjective nature of pain itself. This is especially true for Complex Regional Pain Syndrome cases (“CRPS”). CRPS, formerly known as Reflex Sympathetic Distrophy Syndrome (“RSD”), is an incurable chronic pain condition that is often debilitating. For trial lawyers and their clients, this disorder is especially troubling because of the controversy surrounding its diagnosis and treatment. As its very name implies, the disorder is “complex” in nature, is routinely misdiagnosed, and as such, is difficult to explain and prove to a jury.
Take a recent case that had a mixed diagnosis: Some doctors thought it was CRPS, while some did not. In the end, what mattered was our client had severe pain that would likely afflict him for the rest of his life. This was something the jury understood, whether we called it CRPS or not. The primary purpose of this article is to explain the basics of CRPS, highlight some of the challenges in dealing with a CRPS case, and discuss some useful strategies from a recent trial.
CRPS – WHAT IS IT?
CRPS is a chronic pain condition most often affecting one of the limbs (arms, legs, hands, or feet), in which the pain is out of proportion to thc injury. There are two designations of CRPS: Type I and II. Typc I, which this article will focus on, is a result of trauma. Type II stems from a specific injury to a nerve.
Some researchers have said CRPS is potentially the worst chronic pain disorder a human being could endure. Doctors describe the severe cases of CRPS as being higher on the pain scale than childbirth and amputation. However, over the years, pain management practitioners were overzealous in diagnosing chronic pain patients with CRPS. In the early 1990s, “RSD” cases were popping up everywhere, perhaps in part due to the unclear diagnostic criteria at the time. Now, after the hype has calmed and thorough research has flushed out a more clear understanding of the disorder, CRPS cases can and should command the same attention as other severe injuries such as brain and spinal cord injuries.
To begin with, CRPS arises typically after an injury or trauma to the affected limb. For example, a seemingly simple fracture to the ankle eventually causing a severe pain disorder in that limb. The most frightening aspect of the disease is that it often initially begins in an arm or a leg and often spreads throughout the body. In fact, according to the National Institute of Health, 92 percent of patients state that they have experienced a spread, and 35 percent of patients report symptoms in their whole body.
CRPS is characterized by prolonged or excessive pain and mild or dramatic changes in skin color, temperature, and/or swelling in the affected area. These signs can be subtle in nature, or dramatic, depending on the severity of the CRPS.
CRPS symptoms vary in severity and duration. The key symptom is prolonged pain that may be constant and, in some people, extremely uncomfortable or severe. The pain may feel like a burning or “pins and needles” sensation, or as if someone is squeezing the affected limb. The pain may spread to include the entire arm or leg, even though the precipitating injury might have been only to a finger or toe. Pain can sometimes even travel to the opposite extremity. There is often increased sensitivity in the affected area, such that even light touch or contact is painful (called allodynia).
People with CRPS also experience constant or intermittent changes in temperature, skin color, and swelling of the affected limb. An affected arm or leg may feel warmer or cooler compared to the opposite limb. The skin on the affected limb may change color, becoming blotchy, blue, purple, pale, or red. As discussed in more detail below, due to the complexity of the disorder, CRPS cases are often overlooked, misdiagnosed, and not properly worked up.
VETTING A CRPS CASE
As trial lawyers, we appreciate that many of our clients do not have the type of medical treatment and insurance required to get a complete medical workup and diagnosis. Often, an injury like a brain bleed or spinal fracture might go misdiagnosed. With a disorder such as CRPS, this is truly one of the injuries that often require an attorney’s eye and attention to appreciate the client’s dilemma.
The following are a few points to consider when interviewing a client to determine if he or she potentially has CRPS:
• An injury causing pain which is out of proportion to injury,
• Changes in skin texture on the affected area; it may appear shiny and thin,
• Abnormal sweating pattern in the affected area or surrounding areas,
• Changes in nail and hair growth patterns,
• Stiffness in affected joints,
• Problems coordinating muscle movement, with decreased ability to move the affected body part, and,
• Abnormal movement in the affected limb (most often fixed abnormal posture, or tremors of the affected limb).
For a full CRPS potential case checklist, please contact the author.
Spencer Lucas is a trial lawyer at Panish Shea & Boyle and specializes in complex catastrophic personal injury, products liability and wrongful death cases. He has extensive experience in cases involving traumatic brain injuries, spinal cord injuries, and chronic pain.
Panish Shea & Boyle, LLP
11111 Santa Monica Blvd #700, Los Angeles, CA 90025
•Significant cortical thinning in the prefrontal cortex was observed in CRPS patients.
•Patients with CRPS made significantly more perseverative errors on the WCST.
•Patients with CRPS showed significantly longer stop-signal response time.
•The alterations may explain executive dysfunction and disinhibited pain perception.
Abstract
Few studies have examined the involvement of specific sub-regions of the prefrontal cortex in complex regional pain syndrome (CRPS). We analyzed cortical thickness to identify morphological differences in local brain structures between patients with CRPS and healthy control subjects (HCs). Furthermore, we evaluated the correlation between cortical thickness and neurocognitive function. Cortical thickness was measured in 25 patients with CRPS and 25 HCs using the FreeSurfer method. Pain severity and psychiatric symptoms were assessed using the Short Form McGill Pain Questionnaire and the Beck Depression and Anxiety Inventories (BDI and BAI), respectively. Neurocognitive function was assessed via the Wisconsin Card Sorting Test (WCST) and the stop-signal task (SST). The right dorsolateral prefrontal cortex (DLPFC) and left ventromedial prefrontal cortex (VMPFC) were significantly thinner in CRPS patients than in HCs. CRPS patients made more perseveration errors on the WCST and had longer SST reaction times compared with HCs. Although BDI and BAI differ significantly between the groups, they were not correlated with cortical thickness. Our study suggests that the pathophysiology of CRPS may be related to reduced cortical thickness in the DLPFC and VMPFC. The structural alterations in DLPFC may explain executive dysfunction and disinhibited pain perception in CRPS.
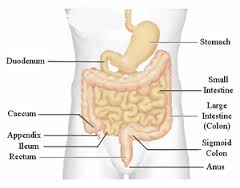
On April 1st I had another procedure to assist in finding out why the symptoms in my belly have worsened over the last year. It wasn’t a routine procedure. Prior to 2013, I was having upper stomach pain that came and went. Held at a 3/4 on average and would rise to a painful 8/9 until I ended up in the Emergency Department at a hard 10 and was admitted for emergency surgery to remove my grossly diseased Gall Bladder. So that I don’t go back into all that, those posts can be found here and ending here for the most part. My stomach never did get better. I was diagnosed with Gastritis during the ERCP in 2013 after my first Gall Bladder surgery, so I knew I had the issue of inflammation around the stomach lining. Reducing fat intake didn’t seem to make a difference, but I’ve kept to low to no fat on a regular basis. My kidney’s are no longer in the greatest shape, but they are functioning. The issues that took me back to the same Gastroenterologist was bleeding, pain, and months of diarrhea, after years of constipation. My tailbone has been clicking in and out-of-place for over a year more and more frequently. Worse when getting up from a sitting position or when on the toilet. I thought it might be due to the Osteoarthritis of the Lumbar Spine diagnosis I’ve had.
I knew I could also feel something inside me when going to the bathroom. As it turns out there was and it was removed during the Colonoscopy. I was diagnosed with Diverticulosis in the recto-sigmoid colon and in the sigmoid colon with colonic spasm. The 3 mm polyp in the sigmoid colon was resected and retrieved. Internal hemorrhoids were found as well, I think many of us have those, either internal or external. Either from constipation, strain or from having babies. I haven’t received the biopsy results yet. I am not worried about that, I’m just glad to have the annoyance out of me. Severe diarrhea has complicated things to the point my legs have a hard time carrying me to the bathroom several times a day and during the night. It’s unfortunate that sometimes there hasn’t been time to get there and I’m closest to the bathroom I can be. That symptom still nags me. I’ve been relying on my Spinal Cord Stimulator even more using it to mask the discomfort around my mid section as well as my legs. Newer reports suggest fiber isn’t as beneficial as previously thought but that mesalamine might be. This September 2014 Mesalamine for Recurrent Diverticulitis Prevention: Results from Phase 3 Controlled Trials report doesn’t seem promising. Everything else is invasive at the critical point. I gained a horrible amount of weight the last 2 years with little to no change in activity or eating habits. Swelling in my face is often, gray color to my facial appearance, a look of black eyes. My stomach extends to the point of looking like there’s a hill-top on one side or so swollen I’m harvesting a human in there. It makes sense now why the area where my Gall Bladder use to be has never stopped hurting. I’ve learned to deal with it and gastritis, the only time it knocks me down some is during a flare up. What I couldn’t fully grasp was all the extra that sprung up along with it.
Over 14 years of CRPS type 2 from a mid-metatarsal separation. I’ve had several lesions removed from my liver, my kidney’s have declined, my uterus lining is inflamed, diagnosed by ultrasound and surgery, with a suggestion to have a hysterectomy. Stomach lining inflammation, and now colon inflammation confirmed. I’ve had an infection for over 2 years. My white blood cell count has been elevated above normal range. I’ve been treated for high blood pressure for a few years now with Lisinopril and recently put on Hydralazine for when it gets above 180/. Maybe a course of antibiotics will help my belly. I still have to followup. I was given 12 photos of my insides after procedure. I’ve been extremely Vitamin D deficient for years now with only 1 testing where I made it into the normal range. My blood is monitored every 4 months.
I have another report that will be ready on the 15th of the month. This one may have CRPS documented as part of the cause. It was at the feedback session. I underwent those tests awhile ago. Still have a few things to work on in regards to the sleep disorders, narcolepsy, brain, brain stem and other issues, but things are moving a long. I’ve been using an Auto Servo Ventilator for about 3 years for OSA, CSA with Cheyne Stokes. It hasn’t helped with the EDS, it has helped with breathing. It’s ability to record every breath I take, don’t take, deep breaths, short breaths and so much more is amazing.
I don’t contribute everything to CRPS, I know that it is part of what’s going on. If doctors aren’t going to consider them related and document it then how can I? I could never go to a new physician and say my insides are coming apart do to CRPS and them ask “who told you that?” and me say “I did”. I’d get laughed right out of the office or not taken seriously about what really might be true and most likely is. That’s why continued awareness, research, documentation, diagnosis’ and timelines are so important. There are many other’s who have developed similar health issues. If we help educate then eventually documentation will take place. We know there is literature to support internal organs being affected, but hardly any providers recognize it.
I’m not sure yet what the plan will be. I should know more this upcoming week. I need to verify too. My procedure photos I came home with are copies. In the copies it shows areas of white outs, white space and white dots, so on film that would look different. I need clarification. I just keep bleeding. JP drain in 2013 for internal bleeding, a hemorrhage during wait period for second surgery months later and during the surgery and again more bleeding. Hurt, hurt and hurt.
Dr Andreas Goebel, from the University’s Institute of Translational Medicine, explains: We found that patients experienced significant pain relief minutes after a placebo therapy, such as salt water injections, but unexpectedly at a later time, and even with repeated placebo applications, there was minimal or no impact on reducing the symptoms of the condition.”
The results suggest that CRPS will not improve naturally over time, and there is little fluctuation in the pain intensity of the condition.
“At least 50,000 new cases of CRPS are diagnosed in the United States annually.1 Although the incidence rate is subject to debate, a large epidemiologic study from The Netherlands involving 600,000 patients suggests an incidence of 26.2 per 100,000 individuals.”